Table of Contents
ECG
An ECG is a routinely performed investigation in the assessment of a poisoned patient. Usually this is performed to detect sodium channel blockade and QT prolongation, two very important complications of overdose.
Sodium Channel Blockade
Sodium channel blockade is a potentially life-threatening effect of poisoning. Drugs with potential to cause sodium channel blockade in overdose include:
| Antidepressants | TCAs, Venlafaxine |
|---|---|
| Antiepileptics | Carbamazepine, Lamotrigine |
| Antihistamines | Diphenhydramine |
| Antipsychotics | Chlorpromazine |
| Cardiovascular drugs | Propranolol, Flecainide |
| Local Anaesthetics | Lignocaine, bupivacaine, ropivacaine |
| Other | Bupropion, hydroxychloroquine, cocaine, orphenadrine |
Tricyclic antidepressants (TCAs) are the most frequently encountered and best studied sodium channel blocking drugs. Good evidence exists for their treatment with serum alkalinisation. Many other drugs can also cause sodium channel blockade; the role of alkalinisation in these exposures is less clear.
Sodium channel blockade results in the typical ECG features of QRS prolongation > 120ms and a dominant terminal R wave in aVR (R’-wave in aVR >3mm or R:S ratio > 0.7).

All patients with evidence of sodium channel blockade on their ECG should remain on cardiac monitoring until the ECG changes have resolved and it is at least 6 hours following an ingestion of an immediate release preparation or 12 hours following an ingestion of a slow-release preparation.
Management of sodium channel blockade
Sodium bicarbonate provides both sodium loading and serum alkalinisation (which reduces the proportion of drug able to interact with the sodium channel). Evidence for the use of sodium bicarbonate for the treatment of cardiotoxicity is largely based on experience with tricyclic antidepressant (TCA) overdoses.
Treat TCA overdose with cardiotoxicity with sodium bicarbonate 1-2 mmol/kg q5min aiming for a pH of 7.50-7.55. Intubation is required to maintain the pH through hyperventilation aiming for a pCO2 of 30-35mmHg.
The role of bicarbonate therapy for sodium channel blockade with non-TCA agents is unclear. A trial of sodium bicarbonate can be given, but if there is no significant response by 3 mmol/kg, it should not be continued.
Excessive use of bicarbonate is harmful and can result in life-threatening hypokalaemia, hypernatraemia, and alkalaemia.
QT Prolongation
The QT interval is measured from the initiation of the QRS complex to the end of the T wave and largely represents ventricular repolarisation. Prolongation of the QT interval is important clinically as it is associated with life threatening Torsades de Pointes (TdP). QT Prolongation can be due to congenital or acquired causes. Of the acquired causes, drugs are a common culprit – with the usual mechanism being blockade of the inward rectifying potassium channel.
In the poisoned patient, you should consider QT prolongation in any exposure to a QT prolonging agent. Drugs associated with QT prolongation and TdP are listed below (this list is not exhaustive):

QT prolongation without a history of exposure to a QT prolonging drug should prompt consideration for other causes of QT prolongation;
- Hypokalaemia
- Hypomagnesaemia
- Hypocalcaemia
- Congenital QT prolongation
A previous ECG maybe helpful in these cases.
Measuring the QT & plotting on the nomogram
The best approach to measuring the QT is to measure the QT interval in multiple leads and take the median value. Be mindful that computer generated QT calculation is unreliable and should not be used.
Plot the QT on the QT nomogram to determine risk of TdP. Values above the line are at risk of TdP and warrant closer observation.

The QT nomogram has a sensitivity of 97% and specificity of 99% for predicting TdP following toxicological ingestions and has been found to be more accurate in predicting TdP than using Bazett’s QTc of 440ms or 500ms.

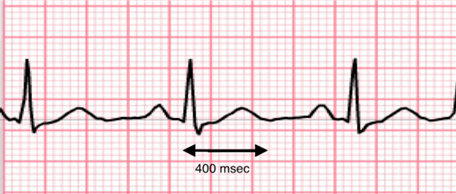
For the above ECG example, the measured QT in leads I, II aVF, V2, V4, V6 are 320, 340, 320, 300, 340 and 320 respectively. This gives a median QT of 320ms. Note the computer-generated QT is longer at 360ms, correcting with Bazett’s formula to 485. However, plotting this on the nomogram shows a level which is well below the risk line.
Bazett’s QTc overcorrects in tachycardia and under-corrects for slow heart rates and should not be used in toxicology patients to determine overall risk of TdP.
Management of prolonged QT
Observe patients with prolonged QT in a monitored environment with continuous telemetry. Review ECGs q4h to follow progression.
Correct modifiable risk factors for TdP:
- Hypoxia
- Hypokalaemia (aim for K+ > 4.5)
- Hypomagnesaemia (aim for Mg2+ > 1.0)
- Hypocalcaemia: (aim for iCa > 1.2)
Management of Torsades de Pointes
Manage as above plus give magnesium sulphate 10mmol (0.1mmol/kg paediatrics) over 10 min, repeat as required. Consider chemical or mechanical overdrive pacing for ongoing stabilisation.
Electrical cardioversion may be required in prolonged cases of TdP – although most cases are self-terminating bursts.
Further Reading
- Bruccoleri RE, Burns MM. A Literature Review of the Use of Sodium Bicarbonate for the Treatment of QRS Widening. J Med Toxicol. 2016 Mar;12(1):121-9. doi: 10.1007/s13181-015-0483-y. PMID: 26159649; PMCID: PMC4781799. PDF
- Isbister G and Page C. “Drug induced QT prolongation: the measurement and assessment of the QT interval in clinical practive. Brit J Clin Pharmacol 2012; 76(1):48-57. PDF
- Thomas S and Behr E. “Pharmacological treatment of acquired QT prolongation and torsades de pointes.” Br J Clin Pharmacol 2015; 81(3):420-7. PDF