Table of Contents
Enhanced Elimination
Overview
Enhanced elimination aims to reduce the severity and duration of an intoxication by increasing the rate at which an absorbed toxin in removed from the body.
As with decontamination the decision to employ these techniques should be on the balance of risk and benefit.
Multi-dose Activated Charcoal
Multi dose activated charcoal (MDAC) enhances elimination through the interruption of enterohepatic recirculation (binding of drugs excreted into the bile before they are reasorbed further along the GI tract) and gastrointestinal dialysis (where lipid soluble, low molecular weight drugs move from gut capillaries back into the lumen down their concentration gradient and bind to charcoal, which in turn maintains the gradient).
MDAC can be considered for a potentially toxic overdose of a drug with a long half-life but small volume of distribution. Complications include constipation, aspiration, and obstruction.
Multiple dosing regimens exist ranging from 25g (0.5g/kg) q2-4h to 10g q1h with ongoing monitoring for abdominal distension and presence of bowel sounds.
Substances amenable to MDAC include:
- Carbamazepine
- Phenytoin
- Dapsone
- Phenobarbitone
- Quinine
- Theophylline
- Cardiac glycosides
- Warfarin
h
Urinary Alkalinisation
Urinary alkalinisation increases the elimination of acidic drugs by increasing the proportion of drug in the ionised state in the renal tubules preventing reabsorption.
Alkalinisation of the urine increases urinary excretion of weak acids (e.g. salicylates, phenobarbitone). This occurs because the two different forms of the acid have different lipid solubility and therefore are reabsorbed by the renal tubules to a greater or lesser extent. As an acid loses a hydrogen ion it becomes ionised and less lipid soluble (HA equilibrates with H+ and A -). Alkalinisation of the urine, by reducing the concentration of free hydrogen ions, causes more of the acid to dissociate to the ionised form to maintain an equilibrium. As the ionised form has low lipid and high water solubility it remains 'trapped' in the renal tubules and is excreted in the urine.
Drugs amenable to urinary alkalinisation should be weak acids (pKa > 3), undergo substantial renal elimination and result in clinically significant toxicity.
Urinary Alkalinisation is used in the management of salicylate and chlorphenoxy herbicide poisoning.
To alkalinise the urine, give 1 mmol/kg (up to 100mmol) sodium bicarbonate bolus followed by an infusion of 25 mmol/h. Place an indwelling urinary catheter and monitor urinary pH q2h, aiming for a pH > 7.5.
Complications include hypokalaemia, hypocalcaemia, hypernatraemia and fluid overload.
Hypokalaemia limits the ability of the kidney to alkalinise the urine. Potassium supplementation (both oral and intravenously) is often required to maintain a serum potassium concentration above 3.5mmol/L.
Regular blood gas analysis can track potential complications (hypokalaemia, hypernatraemia, alkalaemia).
Extracorporeal Techniques
Extracorporeal techniques of elimination are invasive and are reserved for life threatening intoxications which will not respond to supportive care or antidote administration alone.
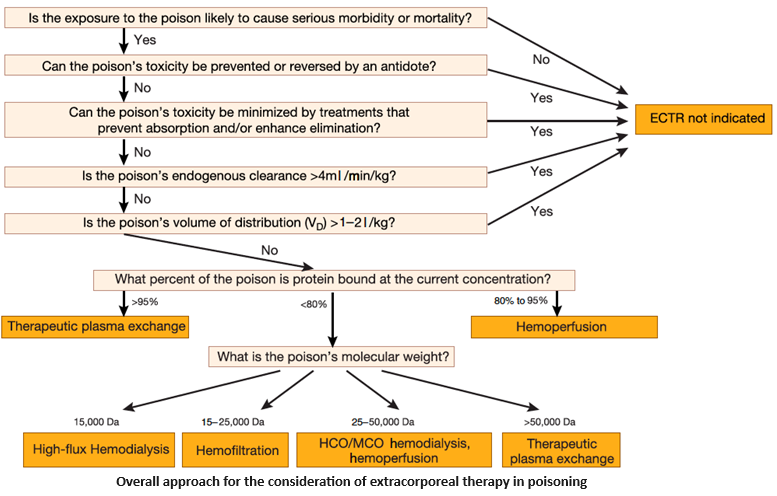
Haemodialysis is the most common technique employed and can be provided in most intensive care units. It is suitable for water soluble toxins which are small, not highly protein bound, with a small volume of distribution. IHD is the preferred mode of haemodialysis where available to manage poisonings, followed by SLED, then CVVHD.
Dialysable substances are usually water soluble, with a low molecular weight, a low volume of distribution and low protein binding. Substances amenable to dialysis include:
- Lithium
- Salicylates
- Toxic Alcohols
- Valproate
- Potassium
- Theophylline
- Lamotrigine
- Carbamazepine
Dialysis is also frequently used following poisoning to support renal failure and to correct acidosis.
Further Reading
- Position statement and practice guidelines on the use of multi-dose activated charcoal in the treatment of acute poisoning. American Academy of Clinical Toxicology; European Association of Poisons Centres and Clinical Toxicologists. J Toxicol Clin Toxicol. 1999;37(6):731-51. doi: 10.1081/clt-100102451. PMID: 10584586. PDF
- Proudfoot AT, Krenzelok EP, Vale JA. Position Paper on urine alkalinization. J Toxicol Clin Toxicol. 2004;42(1):1-26. doi: 10.1081/clt-120028740. PMID: 15083932. PDF
- Ghannoum M et al. ‘Use of extracorporeal treatments in the management of poisonings.’ Kidney International 2018; 94(4):682-688. PDF